IUDs are devices that are inserted through the cervix and sit inside the uterus. The implanon is an implant that is inserted just under the skin of the upper arm and Depo Provera is given by an intra-muscular injection. These are useful contraceptives as they are long-acting (IUDs and implants last 3-5 years), reversible and also very reliable, as the user doesn't have to remember to take a tablet or do anything else once the IUD or implant is inserted, or following their injection.
The Mirena is a commonly used IUD. Apart from being a contraceptive, the Mirena is also very useful for helping to manage heavy and painful periods. The Mirena can be inserted during an appointment with local anaesthetic, however some patients prefer or require insertion of the Mirena under a general anaesthetic in day surgery. After insertion, irregular bleeding is quite common initially, however this usually settles within 3-6 months.
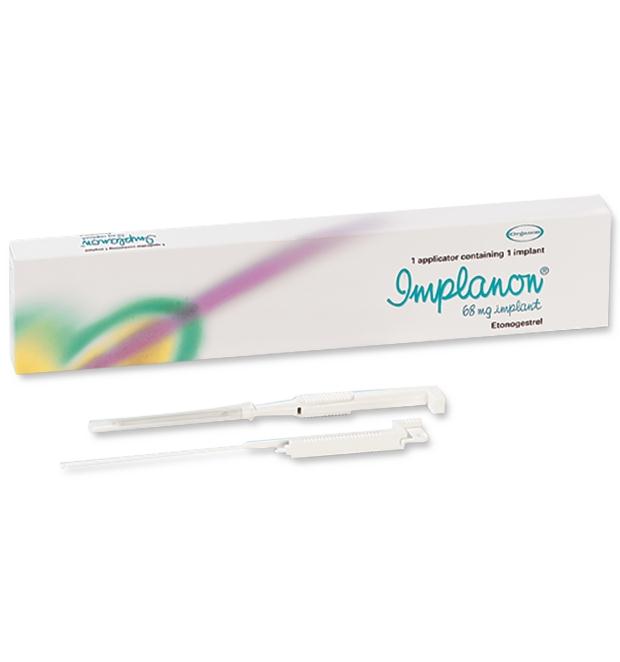
The Implanon is a rod that is inserted just under the skin in the upper arm. It lasts for three years after insertion and, like the Mirena, is a reliable and reversible form of contraception. It also has the side effect of irregular bleeding. The Implanon may be an option for you if you simply need contraception, and prefer not to have the initial discomfort associated with insertion of an IUD.
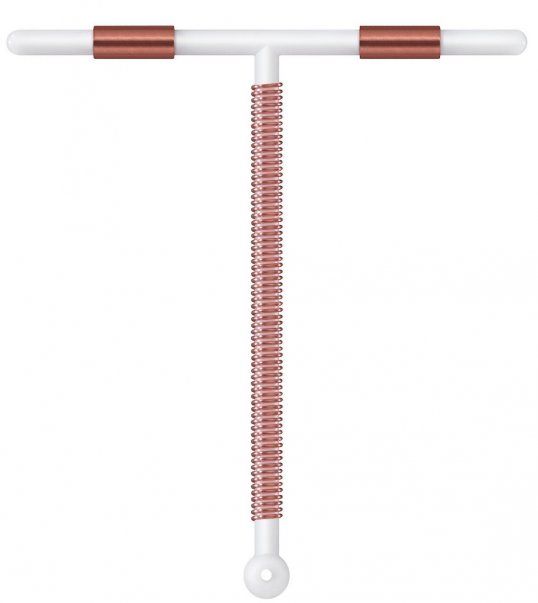
The Copper IUD is another type of intra-uterine contraceptive device, however it does not contain any hormones. Patients who request a Copper IUD may wish to avoid contraceptives containing hormones for various reasons, but at the same time want a reversible and reliable contraceptive option. Sometimes periods can seem a little heavier after insertion of a Copper IUD.
Depo Provera is given by an intra-muscular injection every 12 weeks. Some women cease having periods after using Depo, but it may also cause irregular bleeding. After discontinuation of Depo Provera, some women experience a delay in return to fertility of up to 18 months.
You should seek advice from your GP or gynaecologist before making a decision about whether IUDs, implants or injections are the right contraceptive for you. IUD insertion can be accompanied by some minor discomfort, so if you plan to have an IUD inserted, you may wish to take some Panadol and Nurofen two hours prior to your appointment.
In the next and final Contraception 101, I'll provide an overview of permanent (surgical) methods of contraception.